
Senate Majority Leader Senator Cathy Giessel (R), partnered with Representative Genevieve Mina (D), in a dangerous “pharmacy modernization” experiment (HB 195 & SB 147) that is so wildly beyond their abilities that it would expand Chemical Abortion (Mifepristone) access from Anchorage and Fairbanks Planned Parenthood sites to virtually every city, town, and village that has a hospital, clinic, or pharmacy.
These bills present at least two significant risks to babies and mothers at risk of committing, or being killed by Chemical Abortions:
1. The number of Chemical Abortions will increase exponentially virtually overnight.
2. The number of women seriously harmed by Chemical Abortions will increase dramatically.
What’s at stake with HB 195 & SB 147?
The RU 486 Chemical Abortion Cocktail of Mifepristone and Misoprostol killed 720 babies and sent 79 women to the hospital with serious or life-threatening complications in 2024.
Planned Parenthood operated three abortion sites in 2024. They have since closed their Juneau office, leaving only Anchorage and Fairbanks as primary abortion hubs.
HB 195 & SB 147 could lead to an exponential increase in abortion pill distribution sites from just two in 2026 to hundreds, all across Alaska.
20 additional abortion pill sites, each distributing just one abortion pill kit per week lead to an additional 1,040 babies killed, and 114 women sent to the hospital – or worse.
How The Bills Expand Abortion Pill Access
HB 195 & SB 147 change a few critical parts of existing pharmacy law:
1. HB 195 & SB 147 authorize abortionists and pharmacists to diagnose pregnancies and other health conditions and illnesses under Collaborative Practice Agreements (CPA).
From the bill:
Sec. 6. AS 08.80.337(a) is amended to read:
(a) A pharmacist may, under a collaborative practice agreement with a written protocol approved by a practitioner who is not a pharmacist, provide patient care services. The collaborative practice agreement must define the nature and scope of patient care services the pharmacist may provide under the agreement.
Sec. 7. AS 08.80.337(b) is amended to read:
(b) A pharmacist may independently provide patient care services for
(3) a condition that
(C) requires a new diagnosis only if
(i) the pharmacist uses a test to guide the pharmacist’s diagnosis or clinical decision making;
2. HB 195 & SB 147 redefine patient care services to include prescribing, administering, and dispensing drugs and devices, including abortion pills such as mifepristone.
From the bill:
Sec. 8. AS 08.80.337(d) is amended to read:
(d) In this section, “patient care services“
(1) means medical care services, including the prescription or administration of a drug or device to a patient, that are given in exchange for compensation and intended to achieve outcomes related to the cure or prevention of a disease, elimination or reduction of a patient’s symptoms, or arresting or slowing of a disease process;
(30) “practice of pharmacy” means the interpretation, evaluation, and dispensing of prescription drug orders in the patient’s best interest; participation in drug and device selection, drug administration, drug regimen reviews, and drug or drug-related research; provision of patient counseling and the provision of those acts or services necessary to provide pharmaceutical care; the independent prescribing, dispensing, and administration of drugs in accordance with AS 08.80.168; providing patient care services in accordance with AS 08.80.337; the responsibility for compounding and labeling of drugs and devices except labeling by a manufacturer, repackager, or distributor of nonprescription drugs and commercially packaged legend drugs and devices; proper and safe storage of drugs and devices; and maintenance of proper records for them;
3. HB 195 & SB 147 eliminate much of the Department’s and Board’s approval and oversight of CPAs.
From the bill:
* Sec. 08.02.150. Regulation of collaborative practice agreements.
(a) The department or board may not
(1) require a pharmacist to pay a fee to enter into, or provide patient care services under, a collaborative practice agreement;
(2) require department or board approval of a collaborative practice agreement;
(3) define the nature and scope of patient care services a pharmacist provides under a collaborative practice agreement; or
(4) otherwise regulate collaborative practice agreements.
You can find more about “collaborative practice agreements” under AS 08.80.337(a)
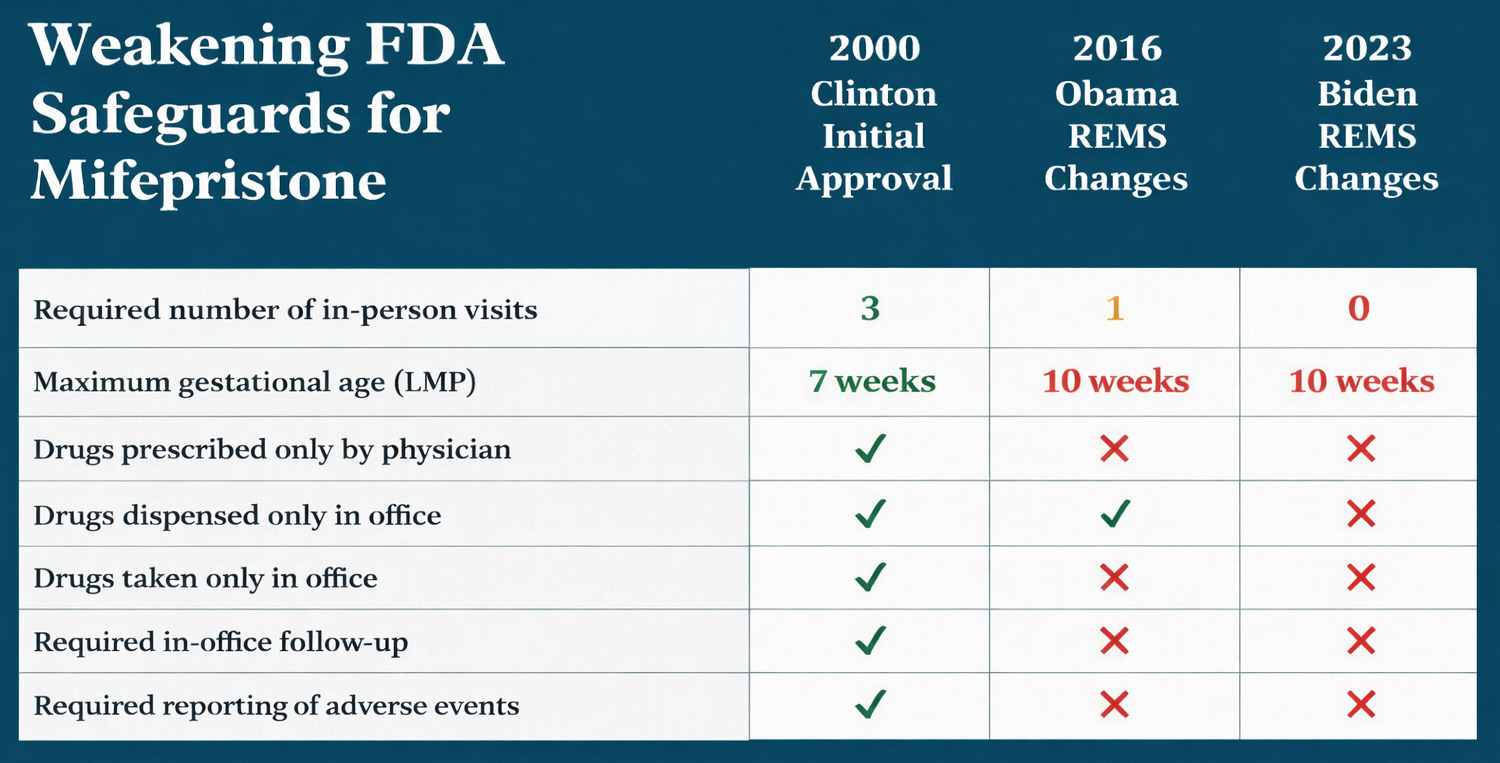
4. The FDA Risk Evaluation and Mitigation Strategy (REMS) for mifepristone has already been relaxed to permit pharmacists’ prescribing and dispensing mifepristone and other progesterone receptor modulators without in person examinations.
{kind=link}
That means a pharmacist can go into business with a medical practice that commits or wants to commit abortions – chemical abortions through a Collaborative Practice Agreement (CPA).
Through that CPA, the abortion business can easily and inexpensively expand its reach into another part of town – or the state.
And because the pharmacist can prescribe and dispense Mifepristone from the pharmacy (or clinic), the cost of expanding the abortion business is minimal.
The only thing left to do is hang advertisements for Mifepristone next to the birth control and early pregnancy test products in the pharmacy or clinic.
And since the demand for Chemical Abortions – Mifepristone – has doubled in the past five years, Alaska’s pharmacies are perfectly positioned to fill that demand.
Chemical Abortions DOUBLED in 5 years
In 2024, 720 babies were killed with Mifepristone/Misoprostol from just two abortion sites.
- 413 more babies died horrific deaths in 2024 than in 2019.
- 42 more mothers suffered from life-threatening complications in 2024 than in 2019.
Chemical Abortions doubled in five years because the Biden Administration made the pills more accessible, women are testing for pregnancies earlier, and the Chemical Abortion pills are perceived to be more ‘convenient than surgical abortions.
Abortion Pill Expansion Champions
HB 195 & SB 147 Sponsors and Champions: Senator Cathy Giessel (R) and Representative Genevieve Mina.
Co-Sponsors include:
Representative Gray (D)
Representative Prax (R)
Representative Story (D)
Representative Eischeid (D)
Senator Gray-Jackson (D)
Voting to ADVANCE the bill(s):
Representative Schwanke (R)
Representative Ruffridge (R)
Representative Saddler (R)
Representative Mears (D)
Representative Mina (D)
Representative Carrick (D)
Representative Hall (D)
Senator Giessel (R)
Senator Claman (D)
Senator Dunbar (D)
Senator Tobin (D)
Voting to ADVANCE without OPPOSITION:
Senator Yundt (R)
Senator Merrick (R)
Senator Bjorkman (R)
Representative Fields (D)
Voting to ADVANCE with AMENDMENT:
Representative Coulombe (R)
Representative Nelson, D. (R)
A Tsunami of Chemical Abortions
What started as a nightmarish 720 babies killed by Chemical Abortions from just 2 Abortion Sites in 2024 is about to become a tidal wave of abortions across Alaska.
Senate Bill 147 & House Bill 195 are companion bills marketed as pharmacy modernization bills that extend prescription authority to pharmacists that is currently limited to physicians, physician assistants, and some nurses.
The bills also expand pharmacies’ dispensing authority to certain controlled substances.
The RU-486 Mifepristone/Misoprostol Chemical Abortion Cocktail can only be prescribed and dispensed in clinical environments in Alaska.
If HB 195 & SB 147 become law, a pregnant mother anywhere in Alaska can complete a telehealth interview with a Planned Parenthood nurse (a 2024 lawsuit expanded chemical abortion prescriptions to physician assistants and some nurses) and have a prescription for Mifepristone / Misoprostol – a Chemical Abortion – sent to the nearest dispensing clinic or pharmacy.
That means a pregnant mother in Kwigillingok, King Salmon, Tok, and even Adak can perform a Do-It-Yourself / Self-Managed Chemical Abortion without leaving her city, town, or village.
HB 195 / SB 147 could legalize more than 300 Chemical Abortion prescription and distribution sites.
Planned Parenthood’s two abortion sites employ only a handful of doctors and nurses that can prescribe and dispense Mifepristone.
Compare that to more than 1,340 Advanced Practice RNs in Alaska that could prescribe and dispense Mifepristone.
Putting this in plain, black and white numbers: Three Planned Parenthood Abortion Sites prescribed and dispensed 720 Chemical Abortions in Alaska in 2024:
Anchorage Planned Parenthood = 540 Chemical Abortions (estimated).
Fairbanks Planned Parenthood = 180 Chemical Abortions (estimated).
What happens when an abortionist in New York sends a prescription to nearly any pharmacy in Alaska?
What happens when Native Health Consortium doctors and nurses prescribe Mifepristone from an Indian Health Services (IHS) telehealth centers and send the prescription to nearly any village clinic to be picked up.
Planned Parenthood’s two abortion sites employ only a handful of doctors and nurses that can prescribe and dispense Mifepristone.
Compare that to more than 1,340 Advanced Practice RNs in Alaska that could prescribe and dispense Mifepristone.
Worse, there are more than 4,100 pharmacists and pharmacy techs working in more than 300 hospitals, clinics, and pharmacies that could either prescribe or dispense Chemical Abortions according to HB 195 / SB 147.
Worse still, phone and internet abortion prescriptions are already available 24 hours / day.
Instead of going to a Planned Parenthood abortion site that’s open 9-5, Monday-Friday, what happens when a pregnant mother can access a tele-health abortionist 24/7/365, and go to the corner pharmacy or village clinic and pick up the Abortion Pills?
Women outside of Anchorage or Fairbanks can go to a local clinic or pharmacy to pick up their abortion prescriptions – no more long drives to Anchorage or Fairbanks for long appointments “just” to pick up the pills.
Perhaps worst of all, Native women in rural Alaska can walk to the village clinic to pick up abortion prescriptions written by a Tribal Health or Native Hospital via tele-health nurse – no more long Medicaid funded trips to Anchorage, Fairbanks, or Seattle “just” to pick up two pills (Mifepristone & Misoprostol).
And all of this while the demand for access to Mifepristone across Alaska is increasing every year.
The possibilities are chilling:
- 13 Rural Hospitals
- 30(+) Federally Qualified Health Centers (FQHC)
- 50 Community Health Aide Program (CHAPS) Clinics
- 100(+) Sub-Regional Clinics
- 50(+) Corner pharmacies and in nearly every store across the state:
- 18 Carrs/Safeway
- 11 Fred Meyer
- 9 Walmart
- 4 Costco
- 4 Three Bears
- 4 Walgreens
How many babies will die when Chemical Abortion pills can be picked up at hundreds of clinics and pharmacies across Alaska?
Every DIY Abortion Pill kills a baby. But the carnage is not limited to the children that die slow, excruciating deaths.
1 in 10 mothers suffers serious to life-threatening complications. In other words, more than 70* women went to the Hospital with serious and even life-threatening complications after killing their babies with Abortions Pills.
The Ethics and Public Policy Center (EPPC) conducted the largest known study on Mifepristone last year based on six years’ of insurance claims data that includes 865,727 Mifepristone abortions. In Alaska, this means:
- 34 Emergency room visits or 4.73% of Alaskan women that have Chemical Abortions
- 24 Hemorrhage or 3.31%
- 20 Surgical abortions to complete botched Chemical Abortions or 2.84%
- 10 Infections or 1.34%
- 5 Hospitalizations or 0.66%
41 Other abortion-related complications or 5.68%
While Danco Laboratories markets Mifeprex (the market name) as “the safe and abortion pill,” Planned Parenthood tells the world that “it’s safer than Tylenol,” and the FDA approved it for use with almost no limitations, the EPPC study found that 10.93% women suffer sepsis, hemorrhaging, infection or other serious complications in the 45 days following a Chemical Abortion.
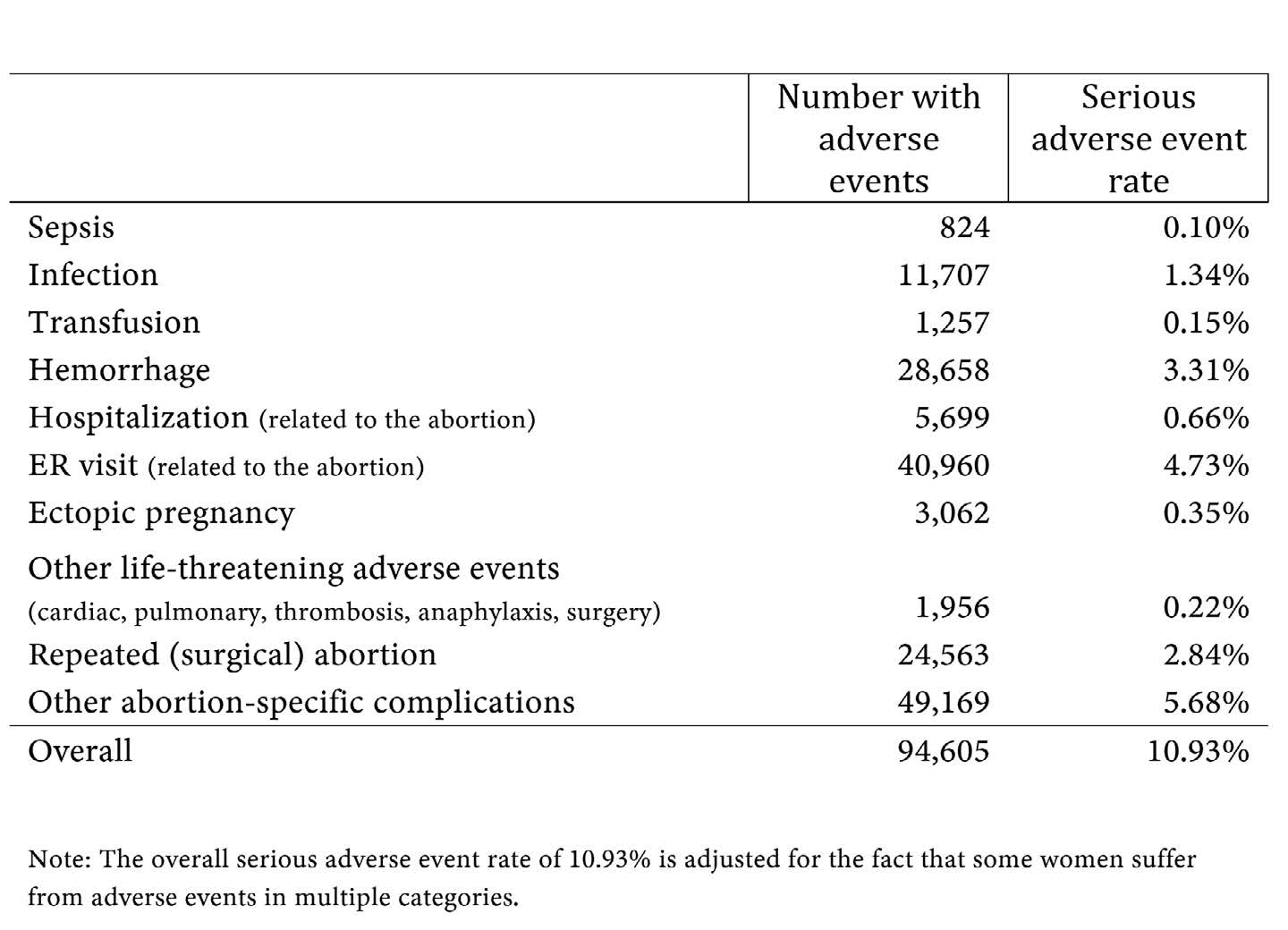
The EPPC Study makes it clear that in addition to claiming the life of a baby, Mifepristone – Abortion Pill – will send nearly 11% of women that take the deadly chemical cocktail to the hospital – or even the morgue.
Every Chemical Abortion kills at least one person – a baby.
1 in 10 Chemical Abortions ends in a serious or life-threatening trip to the Emergency Room – in septic shock, bleeding, infected, or worse.
With the barriers to Mifepristone prescriptions virtually eliminated, the number of women accessing Chemical Abortions will skyrocket.
If the 50 retail pharmacies listed above dispensed just one Chemical Abortion per week, the carnage skyrockets 370% beyond an already unacceptable number of babies killed:
2,600 MORE babies would die horrible deaths.
284 more women would suffer serious to life-threatening complications within 45 days of taking the abortion pills.
- 123 MORE Emergency room visits or 4.73%
- 86 MORE Hemorrhage or 3.31%
- 74 MORE Surgical abortions due to botched Chemical Abortions or 2.84%
- 35 MORE Infections or 1.34%
- 17 MORE Hospitalization or 0.66%
- 148 MORE abortion-related complications or 5.68%
There are also 193 hospitals, clinics and health centers that could prescribe and dispense Abortion Pills across the state.
The number of babies killed by Chemical Abortions alone could reach into the thousands – and the number of women suffering serious and life-threatening adverse events could reach the hundreds!
What happens when a pregnant mother takes the Mifepristone to kill her baby in a remote town or village?
Will a boat, ferry, or plane get her to a distant hospital in time to save her life?
What happens when there is no Emergency Room?
What happens when there is no hospital?
What happens when there is no ambulance?
What happens when there is no help?
If a woman takes an Abortion Pill where boat, ferry, or airplane ride separates her from life-saving treatment, then what happens is she never makes it to the E.R. or hospital?
The EPPC Study does not count deaths – and Big Abortion certainly won’t report abortion related deaths. Without access to hospitals, emergency rooms, blood transfusions, and D&C procedures, how many of those women won’t survive?
I know what you’re thinking: “why haven’t I heard of this before?”
You haven’t heard of this before simply because women in rural Alaska don’t (legally) take Abortion Pills in their towns and villages. That happens in Anchorage and Fairbanks right now.
But if HB 195 / SB 147 become law and they can pick up the Abortion Pills at a rural pharmacy or village clinic, how many more remote abortions will happen, how many more babies will die, and how many more women will suffer serious complications and possibly die because help is too far away?
But remember, this isn’t about “keeping abortion safe,” but about stopping an exponential increase of babies being killed – and the likelihood that many women will die as well.
This is about preventing a radical expansion of Chemical Abortions across Alaska.
This is about protecting desperate mothers and their babies from the predatory lies of Big Abortion and the politicians they employ in our Legislature.
This is about protecting thousands more babies from being murdered by Abortion Pills every year.
Can it get worse?
Big Abortion wants this bill to pass.
Big Pharma really wants this bill to pass.
They have the votes in the House to pass HB 195 / SB 147.
They have the votes in the Senate to pass HB 195 / SB 147.
Without you and thousands like you, HB 195 & SB 147 will become law in 2026.
Pro – Abortion Democrats control the Senate with 6 Planned Parenthood abortion activists, 2 more pro-abortion democrats, at least 6 Republicans supporting the bills – and a binding caucus that commits majority members’ votes to bills they bring to the Senate Floor.
Planned Parenthood abortion activists control 17 seats in the House plus independents and shape shifting Republicans like Stutes – they already have enough to pass the bill without the three Republican votes (Ruffridge, Prax, and Schwanke) already on their side.
Without massive action, HB 195 & SB 147 will sail through the House and Senate.
Here’s the plan:
- Overwhelming Opposition. Senator Giessel and crew will either withdraw the bills or regret every vote on them in 2026.
- Stacks of petition boxes at the Capital steps and on every politicians’ desk.
- Thousands of electronic petitions to every politician in Juneau.
- Hundreds of thousands of emails flooding politicians’ inboxes.
- Thousands of phone calls, bringing the Legislature to a grinding halt.
- Statewide Campaign. Alaska Right to Life members have already sent in hundreds of petitions – and more come in every day.
- Printing flyers.
- Recruiting petition collectors.
- Developing the normal tools for a statewide campaign to defeat these bills.
- Local Action. To protect babies and their mothers from this deadly abortion expansion, we need to defeat these bills in their own districts– and hold their formerly pro-life representatives and senators accountable for advancing abortion expanding bills.
- Church / Pastor Education
- Town Hall engagement
- Literature Drops
- Petition Gathering at Local Events
- Candidate Recruitment
We can’t do any of this without you.
We’re filling politicians’ inboxes with emails and petitions already – but we need more. A lot more.
We’ve already sent more than 5,000 pressure mailers with phone call and petition QR codes into Anchorage and Eagle River – and we’re preparing more for every Republican that’s on the fence.
But we can’t rely on mail and phone calls alone – online education, outreach, and petition recruiting are key components of encouraging Senator Giessel and her colleagues to abandon these wildly dangerous bills.
Here’s what your gift can do right now:
$25 Delivers petitions and pressure mailers to key voters and lawmakers.
$50 Recruits and deliver more petition signatures.
$100 Funds targeted outreach in key Republican districts.
$250 Powers larger waves of mail, digital pressure, and petition deliveries.
$500 Funds on-the-ground outreach and rapid-response mobilization.
$1,000 Expands a full legislative pressure campaign in Juneau.
Please contribute $25, $50, $125, $250, $500, $1,000 or any amount you can afford to help protect pre-born Alaskans and end abortion in Alaska.
We must fully fund this mobilization before the next committee vote – or BIG Pharma and BIG Abortion will lock in the votes they need.
If we fail, Chemical Abortions will spread across Alaska.
If we act now, we can STOP it.
We can’t do any of this without you.
We’re filling politicians’ inboxes with emails and petitions already – but we need more. A lot more.
We’ve already sent more than 5,000 pressure pieces with phone call and petition QR codes into Anchorage and Eagle River – and we’re preparing more for every Republican that’s supporting the bill(s).
We can’t rely on mail and phone calls alone – online education, outreach, and petition recruiting are key components of encouraging Senator Giessel and her colleagues to abandon these wildly dangerous bills.
Here’s what your gift can do right now:
$25 Delivers petitions and pressure mailers.
$50 Recruits more petition signers.
$100 Funds outreach in key Republican districts.
$250 Widens mail, digital pressure, and petition deliveries.
$500 Funds rapid-response mobilization.
$1,000 Expands the Juneau pressure campaign.
Please contribute $25, $50, $125, $250, $500, $1,000 or any amount you can afford to help protect pre-born Alaskans and end abortion in Alaska.
Please contribute $25, $50, $125, $250, $500, $1,000 or any amount you can afford to help protect pre-born Alaskans and end abortion in Alaska.
We must fully fund this mobilization before the next committee vote – or BIG Pharma and BIG Abortion will lock in the votes they need.
If we fail, Chemical Abortions will spread across Alaska.
If we act now, we can STOP it.
Copyright © 2025 · Alaska Right To Life