PP v. State of Alaska
Findings of Fact and Conclusions of Law
Case: Planned Parenthood Great Northwest, Hawai‘i, Alaska, Indiana, Kentucky v. State of Alaska, et al.
Case No.: 3AN-19-11710CI
Source: Uploaded PDF titled “Final Opinion PP v SOA 2024.” This desktop version renders the document as HTML text, not as embedded page images.
IN THE SUPERIOR COURT FOR THE STATE OF ALASKA THIRD JUDICIAL DISTRICT AT ANCHORAGE Planned Parenthood Great Northwest, ) Hawai‘i, Alaska, Indiana, Kentucky, ) ) Plaintiff, ) v. ) ) State of Alaska; et al., ) ) _ _ _ _ _ _Defe_ndan_ts. _ ) ) Case No. 3AN-19-11710CI FINDINGS OF FACT AND CONCLUSIONS OF LAW Introduction Plaintiff Planned Parenthood Great Northwest, Hawai‘i, Alaska, Indiana, Kentucky (Planned Parenthood) filed this lawsuit challenging AS 18.16.010(a)(1), which prohibits anyone other than a licensed physician from providing abortions. Planned Parenthood argues that applying the restriction to otherwise qualified physician assistants and advanced practice registered nurses violates Article I, section one of the Alaska Constitution, which protects the right to equal protection, and Article I, section 22 of the Alaska Constitution, which protects the right to privacy. Planned Parenthood asks the court to enjoin the prohibition on these advance practitioner clinicians from performing first trimester medication abortion and aspiration abortion. The court held a trial to determine whether prohibiting otherwise qualified medical clinicians from providing medication and aspiration abortion substantially burdens patient's fundamental privacy right to make reproductive health care decisions and access abortion care protected by the Alaska Constitution, or violates patients' state constitutional right to equal protection. Based on the evidence presented, the court concludes that, as applied to otherwise qualified medical clinicians, AS 18.16.010(a)(1) imposes a substantial burden on patients' 3AN-19-11710CI Planned Parenthood v. State of .Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
fundamental privacy rights to make reproductive decisions and access abortion care, and their rights
to equal protection,1 and permanently enjoins the State from enforcing AS 18.16.010(a)(1) against
otherwise qualified medical clinicians performing medication and aspiration abortion.2
Course of Proceedings
Planned Parenthood filed a complaint against the State of Alaska challenging AS
18.16.010(a)(1), which prohibits abortion unless performed by a physician licensed by the State
Medical Board.3 The complaint alleges that AS 18.16.010(a)(1) violates the privacy, liberty, and
equal protection rights of patients seeking abortion,4 as well as the equal protection rights of
Planned Parenthood clinical providers whose scope of practice5 would otherwise include
providing medication and aspiration abortion. 6
This court entered a limited preliminary injunction enjoining enforcement of AS
18.16.010(a)(1) with respect to medication abortion after concluding that Planned Parenthood had
demonstrated probable success on the merits of its claims that prohibiting otherwise qualified
clinicians from performing medication abortion violates the privacy and equal protection rights
of patients seeking such care.7
The court also concludes that AS 18.16.010(a)(1) violates the equal protections rights of advanced practice
clinicians whose scope of practice otherwise includes medication or aspiration abortion.
2 See Sagoonick v. State, 503 P.3d 777, 796 & n. 96 (Alaska 2022) ("A litigant may challenge the constitutionality of
a statute or government policy in two different ways. A facial challenge alleges that a statute or policy is unconstitutional
'as enacted'; [the court] will uphold a facially challenged statute or policy 'even if it might occasionally create constitutional
problems in its application, as long as it has a "plainly legitimate sweep." (quoting Planned Parenthood of the Great Northwest
v. State, 375 P.3d 1122, 1133 (Alaska 2016)) (internal citations omitted) An as-applied challenge alleges that 'under the facts
of this case [,] application of the statute [or policy] is unconstitutional. Under other facts, however, the same statute [or
policy] may be applied without violating the constitution."' (quoting State v. ACLU ofA laska, 204 P.3d 364, 372 (Alaska
2009)).
3 Compl. (filed 12/12/2019).
4 ALASKA CONST. art. I § 1, 22.
5 Scope of practice refers to what services or types of care the practitioner is permitted to perform and under what
circumstances. Scope of practice is defined through regulation and also by the education, training, and knowledge of the
practitioner.
,r,r
6 Compl. 111-118.
7 Order on Motion for Preliminary Injunction (entered 11/2/2021).
2
3AN-19-11710CI
Planned Parenthood v. State of Alaska et al.
Findings of Fact and Conclusions of Law
Return to top ↑
Both parties filed motions for summary judgment. 8 This court denied both motions after concluding that there were questions of fact whether prohibiting otherwise qualified medical clinicians from providing medication and aspiration abortion substantially burdens patients' fundamental privacy right to make reproductive health care decisions. 9 ° The court held a bench trial and heard the testimony of five witnesses. 1 Following trial, the parties filed proposed findings of fact and conclusions of law.11 Based on the evidence presented at trial, the court makes the following findings of fact and conclusions of law. Findings of Fact 1. Alaska Statute 18.16.010(a)(1) was enacted in 1970 as part oflegislation legalizing abortion in Alaska. 12 It prohibits abortion unless "performed by a physician licensed by the State Medical Board."13 Knowing violation of AS 18.16.010(a)(1) is a criminal offense punishable by up to five years' imprisonment and a fine of up to $1,000.14 2. Tonya Pasternak, M.D., the Alaska Medical Director for Planned Parenthood and a board certified obstetrician-gynecologist, testified as a hybrid fact and expert witness. As Medical Director, Dr. Pasternak is responsible for ensuring Planned Parenthood's policies and procedures are followed, consultation on complicated cases, physician recruitment and on boarding, training clinical staff, annual reviews of physicians and advanced practice clinicians, coordination of staffing, leadership and strategic planning, as well as direct Plaintiffs Motion for Summary Judgment (filed 12/19/2022); State Defendant's Motion for Summary Judgment (filed 12/19/2022). 9 Order on Cross Motions for Summary Judgment (entered 5/23/2023). 10 11/13/2023-11/17 /2023. 11 Plaintiff's Proposed Findings of Fact (filed 1/26/2024); Proposed Findings of Fact (filed 2/26/2024); Reply in Support of Plaintiffs Proposed Findings of Fact (filed 3/12/2024). 12 Ch. 103, § SLA 1970. 13 AS 18.16.010(a)(1). 14 AS 18.16.010(c). 3 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Pact and Conclusions of LawReturn to top ↑
patient care. She is an expert in the norms and standards for providing gynecological services, including abortion, the practice and training of medical staff, including non physicians, and the scope of practice and competence of advanced practice clinicians.15 3. Dr. Pasternak testified that AS 18.16.010(a)(1) limits the number of days that Planned Parenthood can offer abortion services, placing a burden on patients seeking such care by causing delay, contrary to their health. She testified that AS 18.16.010(a)(1) does not enhance patient safety and instead imposes both a psychological burden and potential medical burdens on patients whose access to abortion is delayed. 4. Dr.Joanne Spetz, Ph.D., testified as an expert in the advanced practice nursing workforce, scope of practice regulations for advanced practice clinicians, and the impact of scope of practice regulations on quality, cost and patient access to care. Dr. Spetz testified that advanced practice clinicians are highly educated professionals who play a growing role in the provision of care in the United States, and that restrictions on scope of practice for advanced practice clinicians are associated with reductions in access to care without benefi.tting quality of care. According to Dr. Spetz, APCs are more likely to accept Medicaid and to practice in community health centers and rural health settings. APCs therefore play an essential role in delivering care for patient populations than are low income, or more isolated or rural. There is a large body of evidence that demonstrates the quality of care, including abortion care, provided by APCs within their scope of practice is comparable to care provided by physicians and that APCs improve access to care. 16 Dr. 15 Advanced practice clinicians (APCs) include advanced practice registered nurses (APRNs) and physician assistants (PAs). 16 Dr. Spetz cited a study of rates of emergency department use following Medicaid expansion. States that permitted nurse practitioners to practice autonomously had very little increases in the emergency department visit rates than states with more restrictions, which experienced steep increases in emergency department visits with Medicaid expansion. 4 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
Spetz testified that AS 18.16.010(a)(1)'s restriction lacks a basis in evidence and research on the safety of APC practice generally and with respect to abortion care specifically, and . . is inconsistent with the way Alaska otherwise regulates the practice of APCs. Dr. Spetz did not conduct research or offer opinions based on data gathered in Alaska, instead basing her opinion on national data or studies in other states. 5. Dr. Shanthi Ramesh, M.D., Chief Medical Officer at Virginia League for Planned Parenthood, testified as an expert in norms and standards for providing gynecological services, including abortion and miscarriage, and in the practical capabilities of medical staff, including non-physicians. Dr. Ramesh testified that AS 18.16.010(a)(1) imposes medically unnecessary restrictions on titime-sensitive health care that could otherwise be safely provided by an APC, limiting access to care. She testified that AS 18.16.010(a)(1) does not benefit patient safety and places additional burdens on patients' financial, logistical, psychological, and physical barriers to care by limiting the number of providers. According to Dr. Ramesh, the licensing and infrastructure of the Board of Medicine and Board of Nursing adequately regulate health care delivery based on medical evidence. 6. Amy Bender, M.S.N., A.R.N.P., F.N.P.-B.C., former lead clinician at Alaska Planned Parenthood, also testified as a hybrid fact and expert witness. At the time of trial Bender had moved out of state but continued to provide telehealth and follow-up care to Planned Parenthood patients in Alaska. In her role as lead clinician, Bender supervised APCs at Planned Parenthood and provided direct patient care. Bender testified as an expert in the provision of reproductive healthcare in Alaska. Bender testified that abortion is within the scope of APC practice, that AS 18.16.010(a)(1) harms patients and does not reflect medical standards or provide any health benefit. 5 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
7. Dr. Ingrid Johnson, Ph.D., testified as an expert in intimate partner violence and rural urban dynamics in Alaska and unique barriers facing victims of intimate partner violence. Dr. Johnson testified that AS 18.16.010(a)(1) increases risk for victims of intimate partner violence to experience exacerbated violence and be unable to receive abortion care within their gestational limit. She testified that barriers for rural victims of violence are more extreme than for other pregnant patients attempting to access abortion. Dr. Johnson testified regarding Alaska's high rates of violence against women, to the increased risk for unintended pregnancy and pregnancy complications for victims of violence, as well as the increased risk of homicide and other violence for pregnant victims of intimate partner violence. Dr.Johnson testified regarding coercive control (including reproductive control) and monitoring behaviors of perpetrators of intimate partner violence that create barriers for victims seeking abortion care. According to Dr. Johnson, in light of those barriers, as well as limited economic barriers and limited social networks, victims of intimate partner violence face significant barriers in accessing abortion care and that AS 18.16.010(a)(1) amplifies those barriers. 8. Planned Parenthood, a not-for-profit corporation, is the only known provider of abortion in Alaska. It operates three health centers in the state, in Fairbanks, Anchorage, and Juneau. Planned Parenthood provides reproductive and sexual health services, including well person examinations, birth control, testing and treatment for sexually transmitted infections, miscarriage care, cancer screening, gender-affirming care, pregnancy testing, and abortion. 9. APRNs include certified nurse midwives (CNMs) and nurse practitioners (NPs). APRNs and PAs hold advanced degrees, have rigorous licensing requirements, and are advanced 6 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
practice clinicians (APCs). Nationally, APCs provide the majority of obstetric and gynecologic care. This is also true at Planned Parenthood's health centers.17 10. Planned Parenthood provides medication abortion at all of its health centers through eleven weeks of pregnancy. It provides aspiration abortion in Fairbanks and Juneau through thirteen weeks, six days, and aspiration and other procedural abortions through seventeen weeks, six days at its Anchorage center. To obtain an abortion after seventeen weeks, six days, a patient must leave Alaska. Planned Parenthood relies on per diem physicians to provide abortion care to comply with AS 18.16.010(a)(1). 11. There are two primary methods of abortion: medication abortion and procedural abortion. In the first eleven weeks of pregnancy patients are eligible for medication and aspiration abortion, a form of procedural abortion. Nationally, approximately 90% of abortions are performed during the first trimester. In Alaska, 89% of abortions take place during the first twelve weeks of pregnancy. 18 12. Medication abortion involves taking medication to end a pregnancy. Medication abortion typically is performed through administration of two medications: mifepristone and misoprostol. Mifepristone blocks the hormone progesterone, which is necessary to maintain pregnancy. Misoprostol, typically taken up to 48 hours after administration of mifepristone, causes the cervix to open and the uterus to contract, expelling the contents of the uterus. Medication abortion does not require instruments, anesthesia, or sedation. Mifepristone and misoprostol are also used to treat miscarriage. 17 At the time of trial, Planned Parenthood currently employed primarily APRNs and contracted per diem with a PA. 1s Based on data from 2020. 7 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
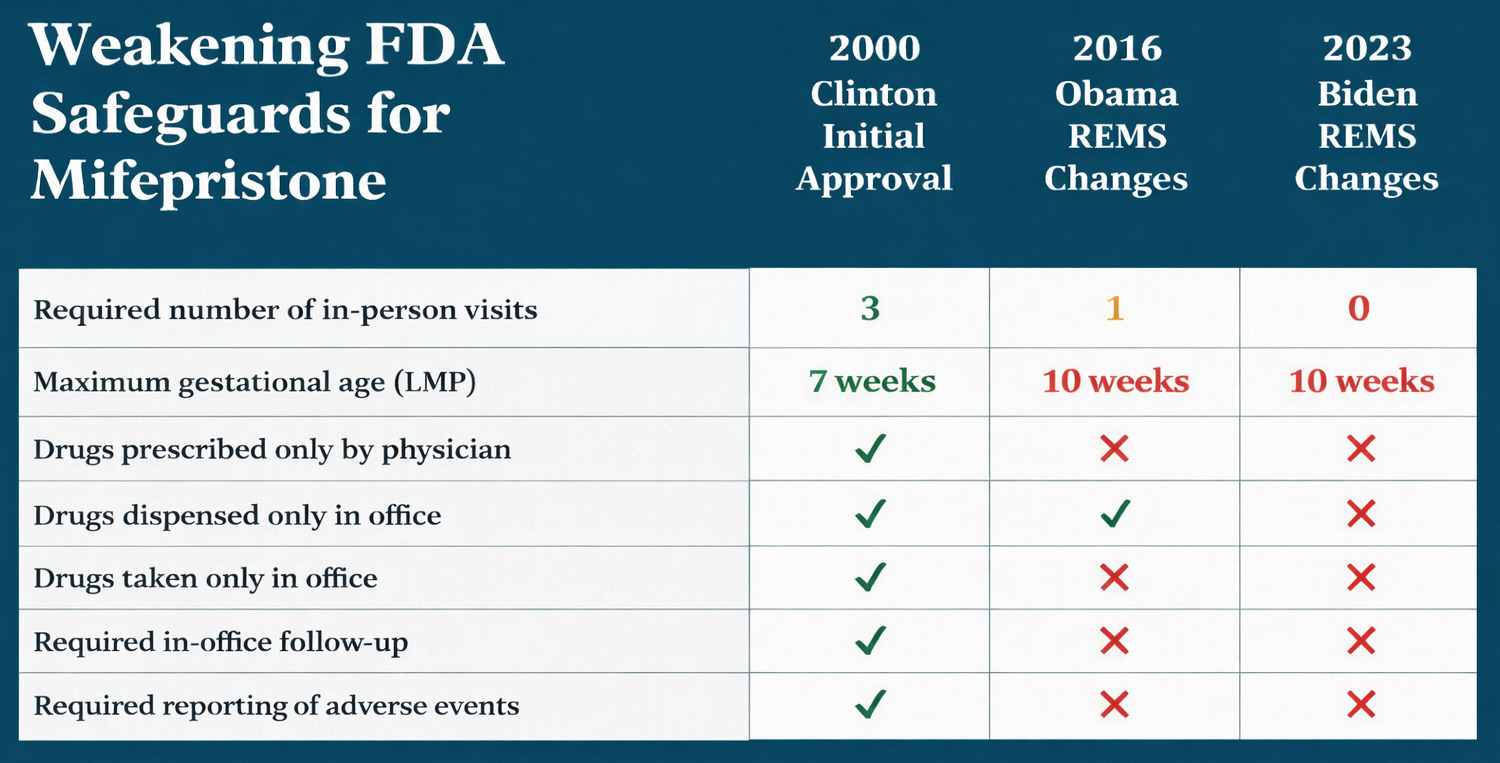
13. The medication regimen was approved by the Food and Drug Administration (FDA) in
2000.19 The initial approval included a requirement of physician supervision (which did
not require the physician to be on-site), later removed in 2016. Between 2019 and 2023
the FDA lifted additional restrictions, including surrounding in-person dispensation and
telehealth. 20 Medication abortion is extremely safe, with a major complication rate of .31
percent.
14. In procedural abortion, a provider uses instruments to end the pregnancy and empty the
uterus. Aspiration is a form of procedural abortion and may be performed up to fifteen
weeks. To perform an aspiration abortion, the clinician uses a speculum to visualize the
cervix, dilates the cervi.'{, inserts a tube into the patient's uterus through the cervix and uses
suction to remove the contents of the uterus. Aspiration abortion is not surgery. It is
extremely safe, with a major complication rate of .16 percent. After fifteen weeks patients
seeking abortion care are eligible for a dilation and extraction (D&E) abortion. 21
15. Some patients require aspiration abortion because they are not eligible for medication
abortion due to contraindications such as having an intrauterine contraceptive device
(IUD), ectopic pregnancy, hemorrhagic disorder, anemia, severe liver or kidney disease, or
19 The 2000 approval was of Mifeprex, the brand-name mifepristone.
20 In Alliance for Hippocratic Medicine, et al v. U.S. Food and Drug Admin., 668 F.Supp.3d 507 (N.D. Tex. 2023), a Federal
District Court entered a preliminary injunction enjoining FDA's 2000 approval of mifepristone (as well as FDA's further
actions in 2016 (extending the maximum gestational age from 49 days to 70 days, eliminating the requirement that
misoprostol be administered on-site at a clinic, removing the requirement for an in-person follow-up exam, and allowing
healthcare providers other than physicians to dispense), 2019 (approving a generic mifepristone), and 2021 (removing the
in-person dispensing requirement)) after concluding that the plaintiffs had shown substantial likelihood of success on the
merits of their claim that the FDA 's 2021 authorization of mail or mail-order pharmacy dispensation of mifepristone and
that FDA's 2000 approval of mifepristone through its regulations accelerating approval of new drugs for serious or life
threatening illnesses, 21 C.F.R. § 314.520. (Subpart H), were unlawful. Ultimately the Supreme Court ruled that the
plaintiffs, doctors and medical associations that did not prescribe or use mifepristone but wanted to make the medication
less available for others, lacked standing to pursue their claims. Food and Drug Admin. v. Alliance for Hippocratic Medicine, 602
U.S. 367, 372-72, 385-97 (2024).
21 D&E is a similar procedure to aspiration abortion, but involves the use of instruments in addition to suction to
empty the uterus.
8
3AN-19-11710CI
Planned Parenthood v. State of Alaska et al.
Findings of Fact and Conclusions of Law
Return to top ↑
taking blood thinner medication. Some patients require medication abortion because they are not eligible for aspiration abortion due to contraindications including complex cardiac disease or uterine fibroids. 16. Some patients prefer one form of abortion over the other. Medication abortion allows patients to end their pregnancies in their own home or place of their choosing, and to choose a time that best fits their other obligations. Medication abortion is experienced similarly to miscarriage. Medication abortion also allows a patient to disguise their abortion as a miscarriage, which can be important for patients who wish to keep their abortion private. Some patients who have experienced rape or sexual trauma prefer medication abortion to avoid the trauma of having instruments placed in the vagina or being placed in the position for a pelvic exam with stirrups on the table. Some patients prefer aspiration abortion because the procedure is completed in the health center in the presence of medical staff. 17. The most common complications from medication abortion are excessive bleeding, incomplete abortion,22 failed abortion,23 infection, and allergic reaction (extremely rare). The risk of excessive bleeding increases with gestational age. The most common complications from first trimester aspiration abortion are excessive bleeding, cervical laceration, uterine perforation, and infection. Complications from aspiration are similar to complications secondary to IUD insertion. Complications from medication and aspiration abortion requiring intervention are usually managed by medication and/ or aspiration and very rarely require hospitalization. 22 Meaning not all of the contents of the uterus are emptied. 23 Continuing pregnancy. 9 3AN-19-11710CI Planned Parenthood v. State of .Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
18. Miscarriage occurs in approximately 10% of patients who know of their pregnancy. Miscarriage management involves three types of care: waiting for the body to pass the pregnancy or tissue, medication management, which uses medication to cause the uterus to contract and pass the pregnancy, and an aspiration procedure to remove the pregnancy tissue. Medication management of miscarriage involves the use of mifepristone and • misoprostol in the same dosages as for medication abortion and requires the same provider skills. 24 Incomplete abortion is when a patient has a miscarriage or medication abortion and has not passed all of the tissue, causing cramping and bleeding. Aspiration is typically used to treat incomplete abortion, is similar to aspiration abortion (e xcept it usually requires less dilation of the cervix) and requires the same provider skills as aspiration abortion. 19. Abortion is safer than pregnancy. Approximately half of pregnancy patients experience complications and 10% are hospitalized for complications (this does not include hospitalization secondaty to labor and delivery). Common pregnancy complications include urinary tract infections, hypertensive disorders, worsening of other chronic conditions and mental health conditions. Some of the more serious complications, such as blood pressure and complications related to cardiac disease, manifest later in pregnancy. 20. Abortion is safer than childbirth. Common complications include the need for delivery by cesarean section, a major abdominal surgery requiring hospitalization, perianal lacerations, wound complications, blood pressure issues, and postpartum depression. Mortality rates for patients who carry pregnancies to term are higher than for abortion patients. Alaska 24 Sometimes medication management involves only misoprostol. ll) 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
maternal mortality rates are twenty times higher than the mortality rate of patients who terminate their pregnancies. Patients living in rural communities, patients with lower socioeconomic status, lower educational attainment, chronic medical conditions, or less access to prenatal or postnatal care, as well as Black women are disproportionately affected by high mortality rates. 21. Abortion is ti.time-sensitive health care. The risks of abortion methods increase with gestational age. As pregnancy progresses, the abortion procedure becomes more complex and patients who are delayed in accessing abortion care may experience increased medical risks. In addition, there are gestational age limits for types of abortion, as well as where those services may be obtained. 22. Patients seek to terminate their pregnancies for a variety of reasons. Some have a medical condition that is worsened by pregnancy. Some are in unstable situations with a partner or family. Many patients are already mothers who do not desire additional children or desire to control the ti.ming of additional children. Some patients' pregnancies are the result of sexual assault. Some patients experience inti.mate partner violence and do not want to parent with that partner. 23. Abortion care is typically siloed to providers like Planned Parenthood. Nationally, there are many state-level restrictions on abortion care, there is stigma associated with providing abortion care, and there are institutional barriers such as religious hospitals restricting abortion. As a result, abortion care is mostly available in urban centers where providers are able to live without harassment and threats. Alaska is no different. 24. APC provider categories emerged in the 1960s. APCs hold advanced degrees and have rigorous licensing requirements. In Alaska, APCs' scope of practice is regulated by state 11 3AN-19-11710CI Planned Parenthood v. State of .Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
boards, as limited by the individual knowledge and education of the APC. APRNs in Alaska are authorized to perform any medical diagnosis and treatment within their scope of practice. Like most states, Alaska authorizes APRN s to practice without physician supervision or relationship. PAs practice under the supervision of a physician and may perform any medical procedure within the scope of practice of the physician.25 25. APCs provide medical care autonomously and prescribe medications, including medication such as narcotics, that carry higher risks than abortion. APCs provide the majority of women's health care nationwide. The Alaska Board of Medicine and Board of Nursing recognizes a broad scope of practice for APCs. APCs in Alaska can perform many of the same tasks as physicians, including examinations, diagnosis, treatment, prescription and dispensation of medication.26 26. APCs routinely manage pregnancy and childbirth in Alaska. APCs provide routine prenatal care, screen for and diagnose serious pregnancy complications, manage vaginal deliveries, repair vaginal lacerations, and routinely manage serious complications such as postpartum hemorrhage. At Planned Parenthood, APCs provide a broad range of reproductive health services, including preventative care, cancer screenings, annual exams, pap smears, screenings for sexually transmitted disease, contraception, and ultrasounds. Abortion is the only medical procedure that is otherwise within their scope of practice that APCs are barred from performing in Alaska. 27. But for AS 18.16.010(a)(1), abortion is or would be within the scope of practice of APCs. Properly trained, APCs can provide medication and aspiration abortion as safely as 25 AS 08.64.170(a)(1); 12 A.AC 40.430(a). 26 AS 08.64.170; AS 08.68.850. ., 1 .:., 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
physicians. There are no greater risks of complications from abortion performed by an APC than by a physician. Planned Parenthood APCs routinely treat complications arising from abortion. 28. APCs are authorized to provide medication abortion in twenty states and Washington, D.C., and aspiration abortion in sixteen states and Washington, D.C. In clinics that have physicians, permitting APCs to perform abortion increases the number of clinicians available to provide the service and expands the number and available times for abortion. 29. Planned Parenthood has policies and procedures to ensure competency in the skills its providers utilize, and that its clinical staff only provide care within the boundaries of their skills and training. Planned Parenthood's medical standards and guidelines are regularly updated. 30. Planned Parenthood APCs provide all care leading up to abortion and provide nearly all follow up care and treatment of complications. APCs are more likely than physicians to manage abortion complications because they are at health centers more frequently. Planned Parenthood APCs staff the 24-hour hotline for post-abortion concerns, triaging patient calls, providing follow-up care and treatment, and referring for a higher level of care if necessary. As a result of AS 18.16.010(a)(1), patients can be prevented from receiving abortion from the clinical provider they are familiar with and with whom they have a relationship. 31. Treatment of abortion complications is medically identical to medication and aspiration abortion, and similar to miscarriage treatment. A patient may experience excessive bleeding with medication abortion. An APC can assess a possible incomplete abortion through ultrasound and treat it with medication or aspiration. This is the same treatment used to 13 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
provide abortion or treat miscarriage complications. There is no difference in skill or training required to provide such treatment for incomplete abortion, abortion, or miscarriage management. The doses of medication used for medication abortion are the same as those used for miscarriage management. Similarly, aspiration for miscarriage management is medically identical to aspiration abortion and requires the same skill and training. 32. APCs are authorized to treat miscarriage in Alaska with medication or aspiration, and it is within their scope of practice. Planned Parenthood APCs in Alaska are not currently trained to and do not provide aspiration in Alaska (for miscarriage or to address complications from abortion). There are relatively low numbers of patients requiring aspiration for miscarriage management or for incomplete abortion. In light of this, and because under AS 18.16.010(a)(1) APCs may not perform aspiration abortions, an APC would need to go out of state to gain sufficient experience and practical training to perform aspiration procedures in Alaska. 27 33. Planned Parenthood APCs routinely provide care similar in risk and complexity to abortion care. APCs treat patients for ectopic pregnancies using Methotrexate, a medication that stops a pregnancy from growing. Medication abortion is safer than Methotrexate treatment of ectopic pregnancy. APCs insert and remove intrauterine devices (IUDs), which requires steps similar to aspiration.28 APCs also provide treatment for HIV, and gender-affirming care, which can be more complex than abortion care. 27 At least one Planned Parenthood APC did this but then relocated out of state and is therefore not performing aspiration in Alaska. 28 The clinician may have to visualize and dilate the patient's cervix and insert instruments through cervix into the uterus. 14 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
34. Since the preliminary injunction was entered, APCs have also been providing nearly all medication abortion. Because Planned Parenthood APCs were already extensively trained, some required only minimal training and were able to begin providing medication abortion within a day of entry of the injunction. The safety protocols for follow-up are the same whether the abortion is provided by a physician or APC. 35. Planned Parenthood's complication rate has remained low since the injunction. Complication rates have not changed from when only physicians provided medication abortion, nor has the rate of hospitalizations increased (following entry of the injunction there were no medication abortion complications requiring hospitalization). 36. There is no medical reason why properly trained Planned Parenthood APCs could not continue to provide medication abortion, no medical reason why properly trained Planned Parenthood APCs could not provide aspiration abortion, and no medical reason why abortion is regulated more restrictively than any other reproductive health care. 37. The evidence was not sufficient for the court to quantify, even roughly, the number of patients who, as a result of AS 18.16.010(a)(1), were delayed in accessing abortion care, were unable to obtain a medication abortion or aspiration abortion due to gestational age as a result of the physician requirement, had to leave the state, or were unable to access care at all. The total number of abortions Planned Parenthood performed after the injunction did not rise, suggesting that, notwithstanding AS 18.16.010(a)(1), Planned Parenthood has been able to meet the overall demand for abortion care. And, as discussed in further detail below, wait times for abortion care appear to have increased. 38. Dr. Pasternak's and Bender's testimony regarding AS 18.16.010(a)(1)'s impact on patients seeking abortion care at Planned Parenthood in Alaska was largely anecdotal and 15 3AN-19-11710CI Planned Parenthood v. State of .Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
impressionistic. In their testimony regarding the impact of AS 18.16.010(a)(1), Bender and Dr. Pasternak relied on their experience treating patients, on patient accounts and on accounts of other clinicians regarding patient difficulties with scheduling. Planned Parenthood did not gather or present data regarding individual patients. Individual patient charts reflect information such as whether patients had complicating medical conditions or were victims of assault, but not whether patients had attempted to schedule an earlier appointment. Patients sometimes offer information at appointments about their difficulties scheduling or attending their appointments. But providers do not typically ask patients why they did not get to a health center sooner to access abortion care because it is not relevant to the care they need and providers avoid questions that may come across as judging the patient. 39. Bender and Dr. Pasternak testified credibly regarding their knowledge and experience of patients who were impacted by delay caused by AS 18.16.010(a)(1). This includes patients who scheduled appointments on days a physician was not available because the patient did not decide to terminate the pregnancy until after making the appointment (e ither because they did not know they were pregnant or had not decided), or sometimes due to scheduling errors for patients seeking an abortion at the time they made the appointment.29 Neither witness quantified how frequently this happened, but Bender testified credibly that it was "not infrequent" and that patients reported challenges and concerns regarding their ability to return to the clinic on a day a physician was available. Bender also testified that she 29 Bender had more direct experience with this type of patient interaction, because she could not provide abortion to a patient seeking one and would have to counsel them about needing to return on a different day when a physician was present. As a licensed physician Dr. Pasternak would not be in such a situation with a patient but was aware of such events through her work as medical director. 16 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
encountered situations where the need for a second appointment would take a patient outside of the window for a medication abortion or for eligibility for abortion within the state. Again, she did not quantify how frequently this occurred, but testified that it was "not uncommon."30 Bender also testified that she was aware of patients who were unable to obtain an abortion and continued their pregnancy because they could not return for a second appointment in time. They also testified that, as a result of the preliminary injunction, they have been treating patients with medication abortion at earlier gestational ages overall. 40. The number of patients who experience significant adverse impacts as a result of AS 18.16.010(a)(1) is low, likely very low, compared to the overall number of abortion patients who receive care at Planned Parenthood. Planned Parenthood overcomes the barrier presented by AS 18.16.010(a)(1) through its staffing and scheduling decisions, successfully so in the vast majority of cases. 41. Planned Parenthood does not employ a full-time physician in Alaska. It employs per diem physicians as needed. APCs deliver the majority of other services offered by Planned Parenthood. This model allows Planned Parenthood, a nonprofit, to keep its costs down. The per diem physicians all have other practices with highly variable schedules, and this model results in some variability in scheduling. Scheduling per diem physicians at Planned Parenthood requires consistent assessment and balancing. 30 Bender estimated that prior to the injnnction, one in fifteen patients had concerns about whether they would be able to return for an appointment within gestational limits for medication and that she could think of 20 to 30 patients who ultimately were nnable to get an abortion in the state due to gestational limits. Based on her testimony and prior deposition testimony, these estimates are highly speculative. 17 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
42. Of Planned Parenthood's clinics, Fairbanks is the most difficult to staff with per diem physicians. At times Planned Parenthood has not had a physician provider in Fairbanks and needed to fly providers in from other locations. Flying physicians is difficult because it increases the burnout rate of that physician due to the long day and weather delays can result in rescheduling. To contract with sufficient numbers of per diem physicians to be able to provide abortion services on every day a clinic was open would significantly increase Planned Parenthood's expenses and administrative burdens. 43. Before the preliminary injunctions, Planned Parenthood offered medication abortion approximately one to two times per week at each clinic, depending on physician availability, including by telemedicine. Generally, there were regular days abortion was expected to be available, but schedules varied somewhat in light of physicians' schedules. Aspiration abortion was available less frequently. 44. Plaintiffs Exhibit 1022 is a chart that purports to map out the number of days each type of abortion was available at each health center before and after the injunction. Some of the other evidence admitted at trial conflicted with the information in the exhibit. For example, according to Exhibit 1022, medication abortion was available before the injunction once per week at each clinic. But the other evidence at trial indicated that medication abortion was available more frequently, particularly through telemedicine. While there were preferred days to schedule abortions at each clinic, the days that physician actually staffed the clinics varied and there was therefore not a truly fixed schedule for available days for abortion at each clinic. 18 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
45. Since the injunction, medication abortion is available at Planned Parenthood's health centers every day the center is open. In Juneau, it is available three days per week, in Fairbanks, four days per week, and in Anchorage, si..x days per week. 46. Planned Parenthood offers aspiration once per month in Juneau (typically the third Wednesday of every month) and Fairbanks (typically the first Wednesday of every month) through thirteen weeks six days.31 Planned Parenthood offers procedural abortion, including aspiration, through seventeen weeks six days, once per week in Anchorage (depending on physician availability). The injunction did not change the availability of aspiration. 32 47. Since the injunction, patients seeking medication abortion have more flexibility in scheduling their appointment. While the number of total abortions performed by Planned Parenthood has decreased, the number of medication abortions has increased. Medication abortion increased by approximately 33 percent in the year following the injunction compared to the year before. However, medication abortion has also increased nationwide during the same period and Planned Parenthood changed its protocols to eliminate or streamline follow-up requirements for medication abortion. Medication abortion increased sufficiently in Fairbanks to reduce the number of aspiration abortions such that Fairbanks began offering aspiration once per month, rather than twice. 48. Since the injunction, patients have been able to receive abortion care earlier in their pregnancies. Before the injunction, it was not unusual for a patient seeking medication 31 There have been times that Planned Parenthood offered aspiration abortion twice per month in Fairbanks depending on physician availability. 32 Patients seeking abortion or miscarriage care requiring aspiration still face delays due to physician availability. With respect to miscarriage care, this can increase the patient's risk of infection. 19 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
abortion to schedule an appointment for abortion after the gestational age limit for medication abortion. After the injunction this has occurred less frequently. 49. Patients seeking abortion services face numerous obstacles. Patients need to take time off of work, school, and childcare responsibilities. Patients who reside outside the three cities where Planned Parenthood operates must make travel arrangements. It is not unusual for patients seeking abortion care to need to reschedule their appointments due to the other barriers they face. Limiting the available days on which patients can make appointments can make it more difficult for patients to access care. 50. These limits have a disproportionate impact on people who are low-income, have limited access to transportation, or have inflexible work or caregiving schedules. Many patients must pay for travel and childcare and take time off of work to obtain abortion care. Delays can increase these costs, particularly if the delay results in a patient exceeding the gestational age for aspiration abortion in Fairbanks and Juneau who must then travel to Anchorage. Patients sometimes schedule and reschedule their appointments due to their personal obligations, contributing to delay. 51. It is not unusual for the limited availability of abortion appointments to result in a delay of a week or more. It is also not unusual for a patient to have to return for successive appointments. Prior to the preliminary injunction, a patient seeking medication abortion may be ineligible due to gestational age and have to return on a day a physician is available. When medication and aspiration abortion are available on all the days a health center is open it can significantly reduce the impact of delay, even when patients need to reschedule for their own reasons. 20 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
52. Delays in accessing abortion care can result in patients exceeding the gestational age limit for medication abortion, for aspiration abortion in Fairbanks or Juneau, and ultimately for procedural abortion in Anchorage. This can result in the patient receiving a different form of abortion than they preferred (aspiration v. medication, D&E v. aspiration), it can result in the need for increased travel, including out of state, to access care, or even in the patient not receiving the abortion. 53. Delay in accessing abortion means that the patient must remain pregnant for longer than they would otherwise. This can expose the patient to the increased risks of pregnancy, which can range from nausea and vomiting, delay in receiving treatment for disease such as cancer, or increased medical risk due to other conditions, such as severe heart disease. 54. Patients who want to terminate a pregnancy are less likely to obtain prenatal care. If the patient is unable to terminate the pregnancy, they face increased medical risks due to lack of prenatal care. They may also experience adverse socioeconomic consequences. 55. Patients who unable to access timely abortion care may experience psychological harm. This is particularly true of patients who are pregnant as a result of sexual assault. Pregnant people experiencing intimate partner violence are at risk for increased violence during pregnancy, and delays in accessing abortion care, particularly if the patient must return for additional appointments, may make it more difficult to keep the pregnancy confidential. Limiting the number of days a patient can obtain an appointment can make it more difficult for the patient to maintain the confidentiality of their care. 56. Wait time data reflecting the amount of time, pre-and post-injunction, that elapsed between when a patient made an abortion appointment and when the abortion was 21 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
performed, was admitted at trial.33 The data showed that patients waited a longer time to receive abortion care after the injunction was entered, which does not support Planned Parenthood's assertion that AS 18.16. 010(a)(1) acts as a barrier to patients seeking abortion. But there were other factors, in particular staffing challenges Planned 34 Parenthood faced during and after the Covid-19 Pandemic, that likely contributed to increased wait times. In addition, the wait time data measured the time between when the patient made the appointment and when the patient attended the appointment. But a more accurate way to measure appointment availability is to track the period of time between the date the patient schedules to the next available appointment. In general, there was no reliable statistical evidence presented at trial that would permit the court to draw a conclusion regarding the impact of AS 18.16.010(a)(1) on a patient's ability to timely access abortion care. 57. Planned Parenthood does not have to exclude the possibility that delays in obtaining abortion care result from patient's personal circumstances in order to meet its burden of demonstrating that AS 18.16.010(a)(1) substantially burdens patients' reproductive rights. The question is whether, in the context of the various barriers patients face, AS 18.16.010(a)(1) increases patients' barriers to accessing care. It does. 58. When APCs are barred from providing abortion, there are fewer available providers, fewer appointments, and potential for greater delay. Given the time-sensitivity of accessing abortion care and the way the service is delivered state-wide through three health centers many patients must travel significant distances to reach a health center. 33 Ex. M, T, U, V. 34 The data showed that in 2020 the average wait time was just under eight days. Average wait times increased in 2021, 2022, and 2023, with an average of just over eleven days in 2023. 22 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
59. Patients have a liberty and privacy interest in access to abortion care, in determining the
type of abortion they receive, and in obtaining those services from their preferred qualified
clinical provider.35 AS 18.16.010(a)(1) substantially burdens this right. As a result of AS
18.16.010(a)(1), some patients experience delays in obtaining abortions, some delays result
in those patients no longer being eligible to obtain their preferred type of abortion, some
patients are forced to travel greater distances to access abortion care, including out of state,
and some patients do hot receive abortion care even when they desired to terminate their
pregnancy. Even though the number of patients affected in the foregoing ways is relatively
low, those impacts constitute a substantial burden on a fundamental constitutional right
to reproductive choice. 36
60. Because AS 18.16.010(a)(1) burdens reproductive choice, it "must be subjected to strict
scmtiny and can only smvive review if it advances a compelling state interest using the
least restrictive means of achieving that interest."37 The State has not asserted that it has a
compelling medical, safety, or public welfare interest served by prohibiting otherwise
qualified APCs from performing medication or aspiration abortion. 38 Certainly, the State
has a legitimate interest in the health and welfare of its citizens.39 But AS 18.16.010(a)(1)
is not the least restrictive means of protecting the health and safety of patients seeking to
35 Order on Cross Motions for Summary Judgment *12-14 (entered 5/23/2023). See also Ht!lfman v. State, 204 P.3d
339, 347 (.Alaska 2009) (the right to make medical decisions on one's own behalf and on behalf of one's children is
fundamental); (Valley Hospital Ass'n v. Mat-Su Coalition for Choice 948 P.2d 963,969 (Alaska 1997).
36 See Planned Parmthood oft he Great NorthJVest v. State, 375 P.3d 1122, 1133 & n. 48 (.Alaska 2016) ("A law is measured
for constitutional validity 'by its impact on those whose conduct it affects,' and the proper constitutional inquiry focuses
on 'the group for whom the law is a restriction, not the group for whom the law is irrelevant."') (q uoting Planned Parenthood
qy
ofS e. Pa. v. Casey, 505 U.S. 833, 894 (1992) overruled Dobbs v. Jackson Women's Health O,;g., 597 U.S. 215, 231 (2022)).
31 State v. Planned Parenthood ofA laska, 171 P.3d 577, 582 (.Alaska 2007).
38 CJ Valley Hosp. Ass'n, Inc., 948 P.2d at 969.
39 Gibson v. State, 930 P.2d 1300, 1302 (.Alaska 1997) (rights to privacy and to bear arms not unconstitutionally
infringed by law criminalizing possession of a firearm while impaired by intoxicating substance).
23
3AN-19-11710CI
Planned Parenthood v. State of .Alaska et al.
Findings of Fact and Conclusions of Law
Return to top ↑
terminate their pregnancies. First, AS 18.16.010(a)(1) does not advance the health or safety of patients seeking to terminate their pregnancies. Second, the law already provides for a comprehensive framework regulating the practice of medicine through the Alaska Medical Board40 and the Alaska Board of Nursing.41 AS 18.16.010(a)(1) is not a regulation of medical care, it is a revision of a criminal law prohibiting abortion. 42 The law carries penalties of up to five years in prison.43 61. Because AS 18.16.010(a)(1) burdens reproductive choice and does not serve a compelling state interest using the least restrictive means, AS 18.16.010(a)(1) violates patients' state constitutional right to privacy and may not be enforced against APCs whose scope of practice includes medication or aspiration abortion. 62. The Alaska Constitution '"mandates equal treatment of those similarly situated"' and protects Alaskans' "right to non-discriminatory treatment more robustly than does the federal equal protection clause."44 To analyze a claim under Alaska's equal protection clause, the court "must identify and assess the nature and importance of the competing personal and governmental interests at stake, identify the relevant level of scrutiny for governmental action, and assess the means chosen to advance governmental interests."45 ' 63. AS 18.16.010(a)(1) treats similarly situated patients unequally. It treats pregnant patients seeking the same medical care differently based on the patient's exercise of their fundamental privacy right to reproductive choice. First, the law treats pregnant patients 40 AS 08.64.010-380; 12 AAC 40. 41 AS 08.68.010-850; 12 AAC 44. 42 § 65-4-6 ACLA 1949; am Ch. 103 § 1 SLA 1970. See former AS 11.15.060. 43 AS 18.16.010(c). 44 State, Dep't of Health & Soc. Serus. v. Planned Parenthood ofA laska, Inc., 28 P.3d 904, 909 (Alaska 2001) (quoting Alaska Pacific Assurance Co. v. Brown, 687. P.2d 264,271 (Alaska 1984)); see also State v. Anthony, 810 P.2d 155, 157 (Alaska 1991). 45 See Planned Parenthood of the Great Northwest v. State, 375 P.3d 1122, 1132 (Alaska 2016). 24 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
seeking medication or aspiration abortion differently from pregnant patients seeking medication or aspiration management of miscarriage. Second, the law treats pregnant patients seeking medical care to terminate their pregnancies differently from pregnant patients seeking all other types of medical care. The law burdens the fundamental privacy rights of pregnant patients seeking to terminate their pregnancies and must therefore be subjected to strict scrutiny. It may only be sustained if it is the least restrictive means of serving a compelling governmental interest. 46 64. To be a compelling interest, the interest must be more than legitimate; the State must show that the interest needs to be vindicated because it is actually impaired.47 The State does not argue that it could meet this high burden. As previously mentioned, there exists a comprehensive statutory and regulatory framework to protect health and safety in the practice of medicine. Absent AS 18.16.010(a)(1) it remains unlawful for a person not properly licensed or qualified through education, skill and training to perform medication or aspiration abortion. Practicing medicine without a license is a class A misdemeanor.48 Practicing nursing without a license is a class B misdemeanor.49 The State Medical Board and Board of Nursing have procedures for ensuring that licensees are qualified and to sanction licensees who do not conform to professional standards.50 Because AS 18.16.010(a)(1) does not serve a compelling governmental interest through the least restrictive means, it may not be enforced against APCs whose scope of practice includes medication or aspiration abortion. 46 Id. 47 Id. &n. 88. 48 AS 08.64.360. 49 AS 08.68.340(a)(2). 50 AS 08.64.326-331; AS 08.68.270-275; AS 08.68.360-390. 25 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of Law - - ~ - - - - - - - - - - - - - - - - - - - - - - -Return to top ↑
65. Planned Parenthood also argues that AS 18.16.010(a)(1) violates the equal protection rights of APCs by prohibiting them from providing care within their scope of practice. This claim concerns APCs' right to engage in an economic endeavor within a particular industry, which the Alaska Supreme Court has held "is an important right that the government may impair only if its interest in taking the challenged action is important and the nexus between the action and the interest it services is close."51 The State has not articulated what its interest in AS 18.16.010(a)(1) is, beyond asserting that the enactment was constitutional in 1970. Even if the State's interest was important, the nexus between the action and the served interest is not close, for the same reasons as previously addressed. Accordingly, AS 18.16.010(a)(1) violates the equal protection rights of APCs and may not be enforced against APCs whose scope of practice includes medication or aspiration abortion. 66. Because AS 18.16.010(a)(1) violates the constitutional right to privacy and to equal protection of patients seeking medication or aspiration abortion, and because the law violates the equal protection rights of APCs whose scope of practice includes medication or aspiration abortion, Planned Parenthood is entitled to a permanent injunction enjoining the State from enforcing AS 18.16.010(a)(1) against otherwise qualified APCs. Conclusions of Law 67. AS 18.16.010(a)(1) violates Article I, section I of the Alaska Constitution, as applied to APCs whose scope of practice includes medication or aspiration abortion. 68. AS 18.16.010(a)(1) violates Article I, section XXII of the Alaska Constitution, as applied to APCs whose scope of practice includes medication or aspiration abortion. 51 Laborers Local No. 942 v. Lampkin, 956 P.2d 422, 430 (Alaska 1998) (quoting State, Dep't of Transp.. & Labor v. Enserch Alaska Constr.., Inc., 787 P.2d 624,631 (Alaska 1989)). 26 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
69. Plaintiffs are entitled to a declaratory judgment and permanent injunction enjoining the State from enforcing AS 18.16.010(a)(1) against otherwise qualified APCs whose scope of practice includes medication or aspiration abortion. 70. Plaintiff must file a proposed judgment within ten (10) days of distribution of these findings of fact and conclusions of law. DONE this 4th day of September 2024, at Anchorage, Alaska. Josie Garton Superior Court Judge I certify that on 9 /04/20?4 a copy of the above was mailed to each of the following at their addresses of record: Susan Orlansky Jennifer Sandman WendyHeipt Catherine Humpreville Camila Vega Vanessa Power Veronica Keithley Shannon Bleicher Margret Paton-Walsh Megyn Weigand Jeffrey Pickett Christopher Robison Harriet Milks Elsie Roehl Judicial Assistant 27 3AN-19-11710CI Planned Parenthood v. State of Alaska et al. Findings of Fact and Conclusions of LawReturn to top ↑
Superior Court Opinion 2024
Findings of Fact and Conclusions of Law
Case: Planned Parenthood Great Northwest, Hawai‘i, Alaska, Indiana, Kentucky v. State of Alaska; et al.
Court: Superior Court for the State of Alaska, Third Judicial District at Anchorage
Case No.: 3AN-19-11710CI
Mobile version: No table of comments included. Page 2 contains the only approved highlighted passage.
Yellow highlight with red underline marks the approved highlighted text from page 2. The source opinion does not include separate printed legal line numbers; the narrow left guide numbers the mobile text rows for easier reference.
Copyright © 2025 · Alaska Right To Life